Clinical scenario:
A 42-year-old male presented with the history of fever of two weeks duration. He also complained of a headache and vomiting episodes twice. He denied any history of weight loss, visit to any endemic zone of malaria or contact with sick people or raw milk ingestion.He visited a local doctor who prescribed some antibiotics but fever didn't settle down. One fine day he woke up and found himself blind .He also could not get up from the bed and was brought to our hospital.
Examination:
Conscious, oriented to time place and person.Pulse was 100/min regular and BP was 120/80 mm Hg. Temp was 39 C
CVS: S1 and S2 were heard.There was grade 2/4 Pansystolic murmur radiating to axilla no peri cardial rub. Chest and Abdomen were clinically normal.
CNS: Neck was free and there were no signs of meningeal irritation. Apart from blindness in both eyes, Cranial nerves were normal. There was grade 4/5 power on right side .Sensations were intact.Cerebellar signs were present on right side.
He had a hemoglobin of 12 .3g/dl , leukocytosis 15,000 normal platelet count, and ESR was 36 mm in the first hour. ECG was normal.Trans thoracic echocardiography revealed evidence of mitral value prolapse but no vegetations were seen.
Keeping in view high clinical suspicion of cardio embolic stroke (Fever and murmur )trans esophageal echocardiography( TEE ) was done which confirmed vegetations on anterior mitral value leaflet Fig 1
 |
Fig Echocardiogram showing vegetation on MVP
|
CT scan head revealed 15 mm hypodense lesion left high frontoparietal region with ring enhancement suggestive of the cerebral abscess. There were other multiple abscesses seen in the right occipital lobe . Fig 2 There was no midline shift and the ventricular system was normal. The findings were confirmed by MRI brain.
Staphylococcus aureus was grown from blood culture sensitive to Ceftriaxone.
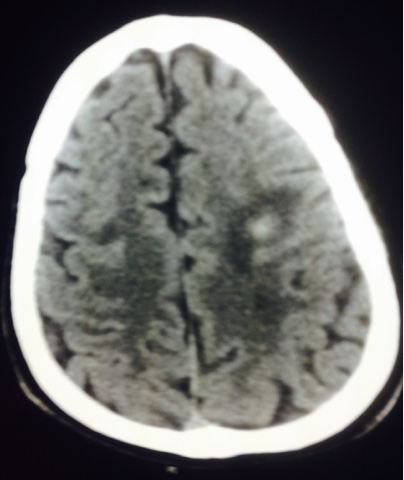 |
Fig 2 CT scan showing infarct Fronto parietal region
|
COURSE :
The patient was managed with 5 weeks parental Ceftriaxone and Vancomycin with regular monitoring of renal function tests.The fever settled.He gradually regained his vision and became ambulatory
Teaching message:
Trans esophageal echo cardiography must be carried out to rule out infective endocarditis when there is high clinical suspicion of cardio embolic stroke i.e a setting of murmur and fever.
This case was contributed by
Dr. Khalid Fathi
Senior Consultant Internal Medicine
King Abdul Aziz specialist Hospital Taif

No comments:
Post a Comment